(412) 586-4678
(412) 586-4678
Hair is composed of strong structural protein called keratin. Keratin - the same strong structural protein that comprises hoofs, fur and feathers in animals and the outermost layer of the skin and nails in humans - is the main protein composition of our hair. Cystine is the most abundant building block of keratin, comprising nearly 25% of the protein. Cystine is a crystallized pair of molecules of the amino acid cysteine.
Each strand of hair consists of three layers.
The most important function of hair in other mammals is that of insulating against cold by heat conservation. In humans, however, we seem to have lost this need over thousands of years of evolution and technological advances (like clothing and hats). Hair subsequently now plays no vital temperature protective role, but scalp hair does offer some protection from the elements and the sun. Other than the filtration function of nasal and ear hairs, an important role for human hair is its participation in the body's sensory system. Sensory nerves surround every hair follicle and any pressure in the area can be felt through these nerves.
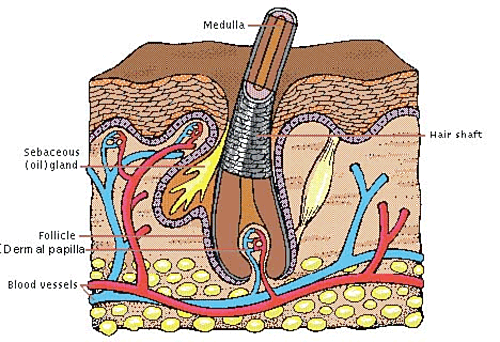
Below the surface of the skin is the hair root, which is enclosed within a hair follicle. At the base of the hair follicle is the dermal papilla. The dermal papilla is feed by the bloodstream which carries nourishment to produce new hair. The dermal papilla is a structure very important to hair growth because it contains receptors for male hormones and androgens. Androgens regulate hair growth and in scalp hair Androgens ma cause the hair follicle to get progressively smaller and the hairs to become finer in individuals who are genetically predisposed to this type of hair loss.
There are four distinctly different types of human hair.
Lanugo are slender downy hairs that begin growing during the second trimester of fetal life and are usually shed before birth. As an infant, we grow short, fine, colorless vellus hairs. Vellus hairs are present over the entire body with the exception of the palms and soles. Following puberty, certain vellus hairs, -those present in the armpits, pubic region, and arm, leg and chest hair in men- may develop in to coarser, thicker pigmented terminal hairs. Terminal hairs are also present on the normal scalp. Those who lose scalp hair often find that hairs, at one time terminal, have become vellus hairs.
On the scalp, where hair is usually densest and longest, the average total number of hairs is between 100,000 and 150,000. Human hair grows at a rate of about 0.5 inch (13 mm) per month.
The typical mammalian hair consists of the shaft, protruding above the skin, and the root, which is sunk in a pit (follicle) beneath the skin surface. Except for a few growing cells at the base of the root, the hair is dead tissue, composed of keratin and related proteins. The hair follicle is a tube-like pocket of the epidermis that encloses a small section of the dermis at its base. The human hair is formed by divisions of cells at the base of the follicle. As the cells are pushed upward from the follicle's base, they become keratinized (hardened) and undergo pigmentation.
Hair follicles grow in repeated cycles. One cycle can be broken down into three phases.
Each hair passes through the phases independent of the neighboring hairs.
Anagen Phase - Growth Phase
Approximately 85% of all hairs are in the growing phase at any one time. The Anagen phase or growth phase can vary from two to six years. Hair grows approximately 10cm per year and any individual hair is unlikely to row more than one meter long.
Catagen Phase - transitional phase
At the end of the Anagen phase the hairs enters into a Catagen phase which lasts about one or two weeks, during the Catagen phase the hair follicle shrinks to about 1/6 of the normal length. The lower part is destroyed and the dermal papilla breaks away to rest below.
Telogen Phase - resting phase
The resting phase follows the catagen phase and normally lasts about 5-6 weeks. During this time the hair does not grow but stays attached to the follicle while the dermal papilla stays in a resting phase below. Approximately 10-15 percent of all hairs are in this phase at an one time.
At the end of the Telogen phase the hair follicle re-enters the Anagen phase. The dermal papilla and the base of the follicle join together again and a new hair begins to form. If the old hair has not already been shed the new hair pushes the old one out and the growth cycle starts all over again.
Each hair passes through the phases independent of the neighboring hairs. Hair is continually shed and renewed by the operation of alternating cycles of growth, rest, fallout, and renewed growth. The average life of different varieties of hair varies from about 4 months for downy hairs to 3 to 5 years for long scalp hairs. Each human follicle follows this cycle independently of others, so the total amount of hair normally remains constant, with an average shedding of 50 to 100 hairs per day lost from a total of around 150,000 follicles.
Everyone experiences some hair loss. This is because hair is shed naturally as part of the normal hair life cycle. As each new hair prepares to grow out from the hair follicle, the old hair is pushed out and shed. Other types of shedding--sudden or excessive loss--are caused by a host of factors, including disease, radiation damage, certain medications, and so on.
Androgens, or male hormones, have a major influence in regulating hair growth. As far back as 400 BC, Hippocrates observed that eunuchs did not become bald, indicating that a male-specific factor was involved in hair loss. Women tend to have less extensive hair loss (also called thinning hair) than men, because women produce lower amounts of androgens which are the primary sex hormones produced in the testes.
Thinning of the hair, or alopecia, occurs in approximately 30-40% of adults, in both men and women. Some causes of alopecia are correctable by treating the underlying problem or by discontinuing the offending agent--such as radiation damage. Causes of alopecia include: thyroid disease, inadequate protein intake, ingestion of certain medications (such as oral contraceptives), cancer chemotherapy, iron deficiency, fungal infections, and improper hair care.
Other causes of thinning hair are generally self-limiting and go away naturally. Causes that are self-limiting include childbirth, high fever, a severe infection, or major surgery. However, alopecia that accompanies chronic illness may persist indefinitely. Certain styling techniques can also cause hair damage, hair loss, and hair-follicle damage. These styling techniques include the excessive pulling (traction alopecia) on hair, such as from straightening curly hair. These damaging techniques also include waxes and hot combs, which harm both hair and hair follicles. Damaged hair follicles may shrink, atrophy, or may die completely. Damaged hair follicles may not be able to regrow hair even after the styling techniques are no longer used.
Men aren't the only ones who have to worry about losing their precious locks. While it may be more common among men, hair loss in women isn't as rare as you might think. It's estimated that hair loss affects 1 in 5 women. The most common types of hair loss are telogen effluvium and alopecia areata. Although it's more common than alopecia areata, telogen effluvium is less severe. This occurs when the hair follicles stop growing and lie dormant and fall out within two to three months. Being that telogen effluvium is oftentimes caused by stress, trauma or medications, hair growth is typically restored within 6 to 9 months. On the flip side, alopecia areata occurs when white blood cells attack hair follicles, causing the hair to thin and fall out, usually in patches. This type of hair loss may require treatment as hair may not grow back on its own.
Your hair says a lot about your overall health. When the body goes into crisis mode, hair growth is stunted to redirect energy to other cells throughout the body. So hair loss is oftentimes the first sign of trouble. While age is definitely a factor of hair loss, other factors, such as hormonal imbalance, emotional stress, medications and hair care products can also lead to thinning of the hair and even male pattern baldness. The best way to get to the root of the problem is to determine the underlying cause.
FPB is a genetic condition that results in hair loss. FPB is caused by hormonal activity. Testosterone in the scalp breaks down, creating Dihydrotestosterone (DHT). DHT causes the hair follicle to atrophy. The conversion from testosterone to DHT is driven by an enzyme called 5-alpha reductase, which is produced in the prostate, various adrenal glands, and the scalp. Over time, the action of DHT causes the hair follicle to degrade and shortens the anagen phase. Female pattern baldness usually begins about age 30, becomes noticeable around age 40, and may be even more noticeable after menopause. Female hair loss is usually an overall thinning (i.e. two hairs where five used to be rather than a bald area on top of the head) though women may have a receding hairline, too. We offer a custom product called DHT Hormone Manager.
Hair loss in women is largely attributed to hormonal imbalance, as it is in men and is one of the lesser known and less common menopause symptoms. Women have more estrogen than men and may help balance out the effects of androgens, namely dihydrotestosterone (DHT), that typically lead to female hair loss.
However, Estrogen can have a variety of complex effects on hair growth: usually, thinning of the hair on the head is a consequence of hypothyroidism. Other hormonal imbalances such as thyroid problems and genetic hormonal responses to autoimmune conditions can also cause thinning of the hair and premature balding in women. In both men and women, loss of hair from the scalp is associated with low thyroid, but “male pattern baldness” has been held to be produced by a male hormone: but even the male hormones can be turned into estrogen by enzymes in the skin, and experiments show that it is estrogen which causes the hair follicle to become inactive, while estrogen-blocker can stimulate the renewal of hair. (R.C. Smar, et al, Proc. Natl Acad of Sciences, Oct 29, 1996).
By suppressing the thyroid and stimulating the pituitary’s secretion of prolactin ( prolactin is a hormone which is known to cause osteoporosis, and which also has a role in breast abnormalities, including cancer). It can suppress the ovaries’ ability to make progesterone, and it affects sweat glands and hair follicles.
We offer salivary and blood spot testing of hormones. Click here to learn about our in-home easy testing modalities.
Lack of iron has long been suspected of contributing to hair loss, but previous experiments did not lead to definite answers because of the insufficient number of subjects studied. A major French study has confirmed the link between iron deficiency and hair loss.
The double-blind, placebo-controlled SU.VI.MAX study, carried out over eight years by researchers at French health and medical institute Inserm, tested the impact of a daily dose of antioxidants on 13000 healthy subjects, including 7886 women, and allowed researchers to provide conclusive evidence that iron deficiency and iron depletion are factors in hair loss. In a questionnaire devised by L’Oréal researchers and distributed to 5000 women participants in the study, more than half of the respondents declared they were concerned by hair loss, and more than 10 per cent described their hair loss as severe.
Data from 3,759 non-menopausal women showed that 48 per cent suffered from iron deficiency or iron depletion. Among post-menopausal women only 23 per cent had lower than normal levels of ferritin because iron loss is often due to menstruation and pregnancy.
Researchers cross-referenced data concerning hair loss and iron reserves, as measured by the amount of ferritin in the blood. They were able to show that non-menopausal women in the ‘severe hair loss’ category had significantly lower iron reserves than women who did not suffer from excessive hair loss. They were also able to estimate the risk of severe hair loss caused by variations in the levels of ferritin. For example, a woman with a ferritin level of 70µg/l (the average level) whose ferritin level falls to 40µg/l has a 28 per cent greater risk of severe hair loss.
Iron deficiency can lead to symptoms such as decreased appetite, lethargy, delays in cognitive or motor development and behavioral problems. However researchers also tend to caution against overdose of the mineral as it has been linked to increased risk of chronic disease in high doses. Proper testing includes Iron and Ferritin. View our product Easy Absorb Iron.
Although women don't have nearly as much testosterone as men, when women undergo intense stress, the adrenal glands become overworked due to an increased need for the "stress hormone" known as cortisol. This causes the body to produce more adrenaline and testosterone, and DHT, a stronger variant of testosterone. The increased production of these hormones can sometimes cause the hair to fall out due to the resulting hormone imbalance.
By stimulating the adrenal glands, (Hans Seleye, known for his discovery of the stress syndrome-and discovered that estrogen duplicated the shock phase of the stress reaction) estrogen can increase the production of androgens from the adrenals that are associated with whiskers and chest hair. (E.C. Ditkoff, et al, “The impact of estrogen on adrenal androgen sensitivity and secretion in polycystic ovary syndrome,” J. Clin. Endocrinol. Metab. 80(2), 603-607,1995) This usually happens when a progesterone deficiency is combined with an excess of estrogen, as in the polycystic ovary syndrome and sometimes at menopause. In animals, polycystic ovaries are caused by a deficiency of the thyroid hormone, and the same regulatory mechanisms seem to operate in women. The PCOS is the most common endocrine disorder in women during the reproductive years, and may occur in 10% of them. (A. Dunaif, et al, eds. The Polycystic Ovary Syndrome. Cambridge, MA: Blackwell Scientific; 1992).
Also, men make progesterone which blocks DHT in prostate and hair follicle.
It's common for women to experience hair loss following pregnancy, when her hormones are in disarray and progesterone levels fall. It takes some time for hormone levels to return to a normal range, so it's perfectly common for post-partum mothers to experience thinning of the hair and even bald patches. In cases such as these, the hair loss is only temporary and treatment oftentimes isn't necessary. Following pregnancy, women can expect hair to re-grow naturally after a few months. If the hair doesn't grow back within the first year, chances are something else is going on.
A variety of medications can result in hair loss in women. Perhaps the most common is birth control. Currently the millions of women use the pill each year, making it the most popular form of birth control to date. According to the American Hair Loss Association (AHLA), it's recommended that women should consider using a low-androgen index birth control pill to avoid the effects of DHT, especially women with a predisposition to hair loss. The AHLA adds that women should exercise caution with any hormonal medication or therapy, as they can all trigger hair loss.
Let's face it: women take pride in their hair. They clean it, color it, cut it, style it, wear it up, down and off to the side. While it may look good now, women should consider the potential damage they're doing to their hair. In addition to brushing, blow-drying and styling, women also use a variety of aerosol sprays, styling gels, chemical straighteners and dyes that not only damage the hair follicles, but also cause irritation of the scalp. If you're experiencing hair loss as result of extreme hair care, your first order of business is to ditch the products that are damaging your hair. If hair growth is not restored within a few months, treatment may be necessary.
If you're suffering from hair loss, chances are a hormonal imbalance is to blame. The state-of the-art at-home tests used by Murray Avenue Apothecary test your female hormones: estrogen, testosterone, progesterone, and thyroid hormones and cortisol to determine if your hair loss is hormonal or genetic. If a hormonal imbalance is the culprit, we will partner with your physician and our compounded bioidentical hormones made in our state of the art lab will help you bring your hormone levels back to optimal balance and effectively treat hormonal hair loss in women.
While you cannot fight your genes, you can fight the effects of aging and hormonal imbalance. Murray Avenue Apothecary partners with physicians who use bioidentical hormones to not only prevent further hair loss, but also to restore hair that you've already lost. Let us help you give your hair what it needs to grow strong and healthy - and soon enough, you'll start getting the compliments you've been missing!
Androgenetic alopecia accounts for 95% of all hair loss. While a person normally sheds 50 to 100 scalp hairs per day, in androgenetic alopecia the rate of hair shedding increases. In women, this condition appears as diffuse hair loss over the entire scalp. In men, the pattern usually starts with a receding hairline, then advances to the top of the head. By the age of 60, two thirds of men will suffer hairloss. This represents some 40 million men in the U.S.. In the U.S. 20 million women are estimated to suffer from hair loss.
The excessive shedding seen with this condition is caused by a shortened growth phase in the hair's life cycle. Scalp and other tissues contain an enzyme called 5-alpha reductase. This enzyme causes a potent male hormone (dihydrotestosterone, or DHT) to be formed in the hair follicle. However, in androgenetic alopecia, genetically primed follicles overproduce the hormone. This shortens the active growth portion of the hair life cycle. Eventually, the shortened life cycle leads to degradation of the follicle. The follicle may die or simply shrink to a size that produces only a fine, unpigmented (vellus) hair. At a certain point, the hair is too thin and fragile to survive, and baldness occurs. See our product Minoxidil.
Alopecia areata affects about 1.7% of the US population. This condition is seen in both men and women, and is often first seen in childhood. There are three types of alopecia areata that affect extensive areas of skin:
Alopecia areata is thought to be caused by an inflammatory response. This inflammatory response is caused by the body's immune system erroneously attacking hair follicles. The attack on the hair follicles causes the hair to enter a resting phase, which is followed by a shedding phase. New hair will not grow until the immune cells cease attacking the follicle. Approximately 20 to 30% of people with alopecia areata have a family history for this condition.
Alopecia areata is self-limiting (will halt on its own) in more than 80% of the cases. In particular, the condition is usually self-limiting when the hair loss occurs after puberty. Hair growth may begin immediately after hair loss, or it may begin again several months to years after the initial manifestation of hair loss.
Treatment for alopecia areata is determined by the extent of hair loss, which is established by your physician. There are four main types of therapy:
Hair growth occurs in cycles, and each hair's cycle is independent of other hairs' growth cycles. This means that individual hairs may be in different stages of life--one hair might be in a growth phase, another in a shedding phase, and other in a resting phase.
Life events can alter hair growth and cause many follicles enter the resting phase simultaneously. A moult or significant shedding will follow such a coordinated resting phase. Such a sudden and shedding of hair may be alarming. Common life-event triggers for moults include childbirth, poor nutrition, some medications, cessation of oral contraceptives, severe illnesses, hemorrhage, surgery, and extreme stress.
Telogen effluvium usually resolves itself over time, without intervention by medication or other therapy. However, scalp-hair density may never return to previous levels.
These conditions are caused by abnormal pulling or twisting of the hair causing breakage of the hair shaft. In these conditions, the scalp is normal (undamaged). When pulling and twisting are stopped, the hair regrows normally unless the follicle has been damaged.
These conditions in children are usually caused by a nervous habit of playing with the hair. Traction alopecia can also be caused by certain styling techniques that pull excessively on the hair, such as straightening techniques.